

- Introduction
- Identification
- Hazard Identification
- Field Detection & Sampling
- Medical Management Overview
- Fire Fighting Measure
- Emergency Procedures
- Protective Equipment
- Containment
- Cleanup
- Decontamination
- Exposure Controls/Personal Protection
- Toxicological Information: Exposure Routes & Health Effects
- Disposal Considerations: Waste Management
- References

FGA Reference Guide (PDF - 789 KB)
Fourth Generation Agents: Reference Guide
(Information as of January 18, 2019)
Introduction
- This guide was developed as part of ongoing preparedness for all hazards and is intended to inform decisions, protect emergency responders, and support response operations if an incident ever occurs involving a fourth generation agent (FGA, also known as A-series or Novichok nerve agents), such as the one used in the United Kingdom in 2018. No illicit use or manufacture of an FGA or other nerve agent is known to have occurred in the United States, and there is no known threat of any nerve agent use in the United States.
- This guide is a supplement to the FGA Safety Awareness for First On-Scene Responders document.
Please visit https://chemm.hhs.gov/nerveagents/FGA.htm for FGA-related resources. - This guide is based on 1) the interpretation of available data on FGAs by U.S. government experts; 2) previously developed federal guidance related to nerve agents; and 3) feedback from local and state emergency responders.
- This guide encompasses a range of potential scenarios involving various methods of FGA dissemination and routes of exposure.
Identification
- FGAs are chemical warfare agents (CWAs) that are unique organophosphorus compounds. They are more persistent than other nerve agents and are at least as toxic as VX.
- If you suspect a potential nerve agent incident, implement protocols for a hazardous materials response and ensure the local FBI Weapons of Mass Destruction (WMD) Coordinator is notified immediately. The FBI will investigate the threat or presence of any nerve agent, including FGAs, as a violation of federal law.
- The National Guard WMD-Civil Support Teams (WMD-CSTs) possess unique training and may perform field identification with specialized U.S. government fielded equipment when assisting local and state responders. Your state Emergency Operations Center can contact the WMD-CSTs if you suspect a nerve agent release.
Hazard Identification
- Entry into an area with known or suspected FGA contamination should be limited to lifesaving activities.
- FGAs are low volatility nerve agents (highly persistent; pose a significant cross-contamination hazard; do not easily evaporate; unlikely to present vapor hazard) and are most likely to be encountered as a liquid. Early recognition may be extremely challenging due to the possibility of delayed onset of symptoms for up to 3 days post exposure.
- The most likely route of exposure is skin contact, but FGAs can also be absorbed into the body by mucous membrane contact (eyes, nose, mouth), inhalation, or ingestion. FGAs may cause rapid or delayed onset of symptoms, depending on the specific agent, dose, and route of exposure.
Field Detection and Sampling
- Detecting FGAs is more challenging than detecting other chemical agents. There is a limited fielded capability within hazardous materials teams to detect, characterize, and identify FGAs.
- M8 paper may be useful in detecting liquid FGAs. Upon exposure to a liquid, a yellow/green or green/blue color is indicative of an FGA, and may shift to a more yellow color over time (up to 10 minutes). This color change is further indicative of an FGA versus VX.
- Failure to detect does not mean that FGAs are not present.
- Monitoring, sampling, and analysis by U.S. government specialized assets may be the only way to determine if FGAs are present. Initial field detection of FGAs may be possible, but more definitive identification of the presence of an FGA will require specialized resources.
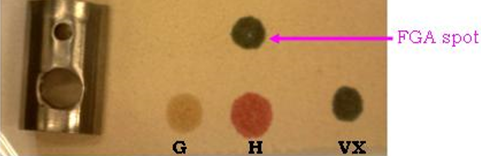
Liquid FGA on M8 Paper — 10 Seconds
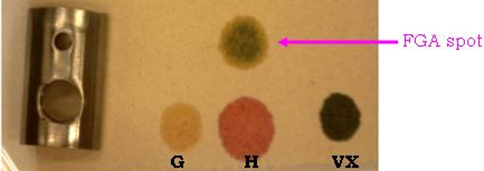
Liquid FGA on M8 Paper — 10 Minutes
Medical Management Overview
- FGAs are more persistent than and at least as potent as other nerve agents. FGAs may require more aggressive supportive care, greater amounts of medication, and a longer duration of treatment.
- Along with supportive care and patient decontamination, the mainstays of managing nerve agent toxicity, including FGA toxicity, are anticholinergics (e.g., atropine), oxime AChE reactivators (e.g., pralidoxime chloride, or 2-PAM), and anticonvulsants (e.g., the benzodiazepines - diazepam, midazolam, and lorazepam).
- See the FGA Medical Management Guidelines (https://chemm.hhs.gov/nerveagents/FGA.htm) for detailed information on treatment.
Fire Fighting Measures
- See Department of Transportation Emergency Response Guidebook GUIDE 153 and guidance for UN2810 VX (Table 1: Initial Isolation and Protective Action Distances).
- Allow fire to continue to burn unless these actions would result in greater risk to the public.
- Use protocols established for organophosphorus pesticides.
- Use dry chemicals, carbon dioxide, alcohol-resistant foam or other foam materials to extinguish fires.
- Fight fire from upwind and uphill, if at all possible.
- Avoid using water to extinguish fires. FGAs are highly soluble in water, will persist, are highly mobile, and could contaminate larger areas.
- Dike fire control water for later treatment and disposal; runoff from fire control or dilution water may be extremely toxic resulting in contaminated water supplies and further complicate clean-up efforts.
- Smoke/steam plume may be contaminated by the agent; large areas downwind of fire may be affected by contaminated smoke/steam plume.
Emergency Procedures
- It is possible responders may perform lifesaving actions prior to recognizing that a hazard, including an FGA, is present. Responders performing lifesaving actions should wear appropriate Personal Protective Equipment (PPE) and minimize the number of personnel entering the potentially contaminated area. Wear eye protection and double layer nitrile gloves. Change your outer layer of gloves as needed using proper donning and doffing procedures.
- In the case of a mass casualty incident where an FGA is suspected, the incident command shall ensure that the PPE worn is appropriate for the hazards to be encountered.
- Report any potential exposure and be medically evaluated immediately per your department or agency’s procedures if you are involved in an incident that includes the presence of an FGA. Symptoms may occur up to 3 days post exposure.
Protective Equipment
- The minimum level of protection should be positive pressure self-contained breathing apparatus (PP/SCBA) and other appropriate PPE until a hazard and risk assessment has been conducted.
- The PPE requirements for FGAs are the same as those for VX. The following levels of protection are recommended for incidents involving FGAs:
- Ensembles certified to National Fire Protection Association (NFPA) 1991 Vapor Protective Ensemble (Occupational Safety and Health Administration (OSHA)/ Environmental Protection Agency (EPA) Level A)
- Ensembles certified to NFPA 1994 Class 1 Hazardous Material and Terrorism Vapor Protective Ensemble (OSHA/EPA Level A)
- Ensembles certified to NFPA 1994 Class 2 Hazardous Material and Terrorism Vapor Protective Ensemble (OSHA/EPA Level B)
- If chemical detection monitoring and hazard identification results confirm the contaminant identity and concentration in air, then ensembles certified to NFPA 1994 Class 3 Hazardous Material and Terrorism Protective Ensemble (OSHA/EPA Level C) can be utilized, provided the airborne concentrations are at a level appropriate for the use of a National Institute for Occupational Safety and Health (NIOSH)-approved Chemical, Biological, Radiological, and Nuclear (CBRN) Air Purifying Respirator (APR) or Powered APR (PAPR).
- When responses involve releases of chemical substances, use a hazard and risk assessment and adhere to Federal OSHA, OSHA-approved State Plan, or EPA Hazardous Waste Operations and Emergency Response (HAZWOPER) standard (depending on which applies).
- Chemical resistant boots and chemical resistant butyl rubber gloves that are at least 14 mil thickness are recommended when dermal exposure is possible. NFPA 1991- and NFPA 1994-compliant ensembles include gloves and boots that provide acceptable levels of protective performance.
- Strict adherence to appropriate PPE donning and doffing procedures is critical. Cross-contamination is a significant concern to emergency responder health and safety in incidents involving FGAs.
- Downgrading PPE levels can be considered only when the identity and concentration of the contaminant is complete and a risk assessment of dermal and inhalational exposure has been performed. Responders should follow their standard operating procedures and guidance of personnel who have conducted a thorough hazard and risk assessment such as hazardous materials technicians, WMD-CSTs, Certified Industrial Hygienists, or other allied subject matter experts.
PPE Protection Levels
|
Level A |
Level A provides the greatest level of skin (fully encapsulating suit), respiratory (SCBA), and eye protection when the contaminant identity or concentration is unknown. Select Level A when the concentration is unknown and when there is a potential of ocular or dermal exposure.
There are two NFPA standards that contain the design, performance and testing methods that provide assurance that certified ensembles that provide adequate vapor protection are consistent with the protective characteristics of Level A garments: NFPA 1991 Standard on Vapor-Protective Ensembles for Hazardous Materials Emergencies and CBRN Terrorism Incidents and NFPA 1994 Standard on Protective Ensembles for First Responders to Hazardous Materials Emergencies and CBRN Terrorism Incidents (Class 1 ensemble). The SCBA should be certified to NFPA 1981 Standard on Open-Circuit Self-Contained Breathing Apparatus (SCBA) for Emergency Services. This SCBA standard contains a mandatory requirement that the unit has a NIOSH CBRN SCBA approval. |
|---|---|
|
Level B |
Level B provides the highest level of respiratory protection (SCBA) when a lesser level of skin protection is required. Select Level B when the FGA concentration is unknown and dermal exposure is less of a risk. Level B differs from Level A in that the chemical protective garment design can be either totally encapsulating or a non-encapsulating, splash-protective, chemical-resistant outer suit that provides protection against most liquids but may not be airtight.
The SCBA should be certified to NFPA 1981 Standard on Open-Circuit Self-Contained Breathing Apparatus (SCBA) for Emergency Services. This SCBA standard contains a mandatory requirement that the unit has a NIOSH CBRN SCBA approval. There are two NFPA ensembles that function in similar manner to Level B garments. NFPA 1994 Class 2 does provide an appropriate level of vapor protection.[1] Only the NFPA 1994 Class 2 garments have been tested and certified against CWA agent hazards. |
|
Level C |
Select Level C when the contaminant identity and concentration are known and the respiratory protection criteria factors for the use of APR or PAPR (e.g., < Immediately Dangerous to Life and Health, < maximum use concentrations, and warning properties) are met. Level C may be appropriate when decontaminating personnel or equipment.
NFPA 1994 Class 3 provides a limited level of vapor protection and can be used with a NIOSH approved CBRN APR or PAPR. |
[1] NFPA 1992 Standard on Liquid Splash-Protective Ensembles and Clothing for Hazardous Materials Emergencies may not provide an appropriate level of vapor protection.
Containment
- Minimize waste generation and segregate types of waste (PPE, liquids, etc.). FGAs can persist for extremely long periods of time on materials and effluent liquids such as water, so treat waste materials as hazardous and extremely toxic.
Cleanup
- Control water used for cleanup for later treatment and disposal. Runoff from fire control or dilution water may be extremely toxic, resulting in contaminated water supplies and further complicating clean-up efforts.
Decontamination
- Cross-contamination can occur between victims and responders. Follow established decontamination procedures.
- Avoid direct contact with runoff water because FGAs are not readily degraded by water.
- According to a statement issued by the EPA, responders generally may prioritize actions to save human lives and protect health. After imminent threats are addressed, responders should immediately take all reasonable steps to contain contamination (including decontamination runoff) and mitigate environmental consequences.
Emergency Decontamination of Victims and First Responders
- Remove clothing and personal effects and place items in a plastic bag. This is a vital step to reduce ongoing and secondary exposure and can remove significant amounts of chemical contamination. Responders should pay particular attention to how clothing and personal effects are removed in order to minimize the spread of contamination.
- Contain suspected or confirmed contaminated clothing and personal effects, by tightly closing bags and double bagging in 6 mil polypropylene bags, if possible.
- Do not break the victim’s skin. Cover all open wounds during the decontamination process.
- Use a paper towel, dry wipe, or other dry cloth to blot (do not wipe) any visible contamination from the skin. This dry decontamination step can be performed by victims themselves and, along with clothing removal, should be done as early as possible. Disrobing and blotting skin with a paper towel, dry wipe, or other dry cloth can remove significant amounts of chemical contamination.
- Reactive Skin Decontamination Lotion (RSDL), if available, is recommended for spot decontamination. RSDL cannot come into contact with bleach. Combustion may occur upon contact with strong oxidizing chemicals (e.g., dry chlorine products like, HTH [calcium hypochlorite powder], super tropical bleach). Do not discard used RSDL components into strong oxidizing chemicals or their containers.
- Water should be utilized per established decontamination protocols after disrobing, ideally with a high-volume, low-pressure shower, including soap if available, gentle rubbing with a soft cloth or sponge, and active drying with a clean towel after the shower. Do not delay decontamination awaiting specialized decontamination products such as soap or RSDL. FGAs can remain toxic in the wash water; treat it as contaminated waste.
- Avoid using hand sanitizer or other products containing alcohol, as they may enhance absorption of the agent and spread it over a larger area of the victim’s skin. Do not use bleach to decontaminate skin.
Caring for Victims after Emergency Decontamination
- Move the victim to a casualty collection area where ongoing evaluation and emergency medical treatment can be provided.
- Coordination with the hospital(s) prior to transport is necessary to ensure that the hospital(s) knows the victims have been exposed to an FGA and confirm an isolation/decontamination receiving area and proper PPE are available.
- If the victim was transported without being decontaminated, the ambulance or other transport vehicle should be considered contaminated. Steps should be taken to prevent further contamination of victims and equipment.
- See the FGA Medical Management Guidelines (https://chemm.hhs.gov/nerveagents/FGA.htm) for additional information related to decontamination in a hospital setting.
Technical Decontamination of Entry Teams
- A decontamination line suitable for CWAs/FGAs for responders entering the exclusion zone should be established.
- Refer to your department or agency’s standard operating procedures for technical decontamination procedures for nerve agents.
- Double bag all PPE and equipment in labeled, durable 6 mil polyethylene bags.
- All equipment that has been potentially contaminated by FGAs should be set aside; consult with experts for current decontamination or disposal recommendations.
Exposure Control/Personal Protection
Exposure Limits
- The U.S. government has no occupational exposure data on FGAs. There are no established occupational exposure limits, Permissible Exposure Limits, or Acute Exposure Guideline Levels for FGAs, so all precautions must be taken to prevent any exposure. The recommendations in this guide are based on the reported toxicity and the chemical and physical properties of FGAs.
Physical and Chemical Properties: FGA General Characteristics
|
Vapor Pressure |
Extremely low vapor pressure; 5 to 10 times lower than VX |
|
Density (vapor) |
Heavier than air |
|
Skin Absorption |
Easily absorbed by the skin |
|
Aqueous Solubility |
Highly water soluble |
|
Soluble in |
Acetone, benzene, ethanol, methanol, chloroform, saline |
|
Flash Point |
Greater than 300 degrees Fahrenheit |
|
Persistence |
Can remain on environmental surfaces for days or even many months, if not decontaminated |
Toxicological Information: Exposure Routes and Health Effects
Exposure Routes
- The most likely route of exposure is skin contact, but FGAs can also be absorbed into the body by inhalation, mucous membrane contact (eyes, nose, mouth), or ingestion. After exposure, symptoms may occur within minutes to hours or up to 3 days. Prompt administration of decontamination procedures and medical evaluation are critical.
Signs/Symptoms
- The presentation and timing of symptom onset depends on the agent, dose, and route of exposure. Regardless of the route of exposure, patients may demonstrate some combination of SLUDGE and DUMBBELS.
SLUDGE – Salivation, Lacrimation, Urination, Defecation, Gastrointestinal upset, Emesis
DUMBBELS – Defecation, Urination, Miosis/Muscle weakness, Bronchospasm/Bronchorrhea, Bradycardia, Emesis, Lacrimation, Salivation/Sweating
- Seizures, coma, and death may occur in severe exposures.
Disposal Considerations: Waste Management
- Waste management should immediately be considered when generating waste. Once the incident is determined to involve FGAs, responders should minimize waste generation and segregate types of waste (PPE, liquids, etc.). FGAs can persist for extremely long periods of time on materials and effluent liquids such as water, so treat waste materials as hazardous and extremely toxic.
- Waste should be secured for law enforcement purposes prior to disposal.
- PPE, equipment that cannot be adequately decontaminated, and other material that has been contaminated by the nerve agent should be disposed per an incident specific waste management plan which may include incineration or other approved methods.
- Once the lifesaving efforts are under control, the incident command, along with a site-specific health and safety plan, should develop a comprehensive waste management plan prior to any formal cleanup.
- Consult with experts for disposal recommendations.
References
- Guidance on Emergency Responder Personal Protective Equipment (PPE) for Response to CBRN Terrorism Incidents (CDC/NIOSH)
- Hazardous Waste Operations and Emergency Response (HAZWOPER) (DOL/OSHA)
- Emergency Response Safety and Health Database VX: Nerve Agent Card (CDC/NIOSH)
- Best Practices for Protecting EMS Responders during Treatment and Transport of Victims of Hazardous Substance Releases (DOL/OSHA)
- Best Practices for Hospital-Based First Receivers of Victims from Mass Casualty Incidents Involving the Release of Hazardous Substances (DOL/OSHA)
- Primary Response Incident Scene Management (PRISM) Decontamination Guidance for Chemical Incidents (HHS/ASPR/BARDA)
- Emergency Response Guidebook (2016), GUIDE 153 and Guidance for UN2810 VX in Table 1 for Initial Isolation and Protective Action Distances (DOT)
- First Responders’ Environmental Liability Due to Mass Decontamination Runoff (EPA)